

The Sunday Times - NHS efficiency suffers from a rash of data rules January 14th 2018 - 12 Downloads
The Sunday Times - NHS efficiency suffers from a rash of data rules
14th January 2018, David A Rew, Consultant Surgeon
Sir, Camilla Cavendish cogently identifies the NHS as 700 separate entities rather as a functional superpower (“Call Dr Stalin: the NHS must be forced to unify”, Comment, last week). This Balkanisation applies particularly to information flows.
We have developed and implemented at negligible cost to the taxpayer an electronic patient record that integrates the general practice, hospital and social care records in a single format. This could then be easily understood and used by every health and social care professional, subject to appropriate access controls.
Unfortunately, like a caged tiger, our system is unable to reach its full potential in wider testing because partner NHS organisations, GPs and other care providers are constrained by the overpowering bureaucratic rules and regulations around data security, which also protect closed data empires.
Most citizens would presumably prefer and expect to see their critical healthcare information flow seamlessly and responsibly around a simpler national health and social care data estate. At present, information remains pointlessly guarded in silos at hugely wasteful cost to the taxpayer and at morbid cost to the citizen in need of joined-up care.
David Rew, consultant surgeon, University Hospital of Southampton
Background
The previous weekend, Camilla Cavendish had written a very insightful article on the disjointedness of the NHS information systems, which I have reproduced in full below. This reflected my own frustrations at the difficulties which we were facing in securing NHS digital engagement with a radical approach to information integration and efficiency, UHS Lifelines, which I have written about extensively elsewhere, and which is illustrated below:
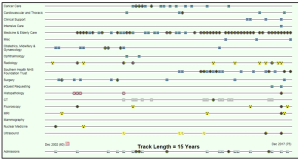
Image: A screenshot of the live patient record as rendered in the transformative UHS Lifelines interface which we had built in Southampton. Each icon on each timeline is a window to the underlying document or event for that patient. This was the output of the system to which I allude in my letter to the Sunday Times
Call Dr Stalin: the NHS must be forced to unify
Cash is not enough — the only cure is a properly joined-up health service
Camilla Cavendish; The Sunday Times January 7th 2018
Everyone in the NHS dreads the first week of January. Norovirus and flu stalk the land. Revellers clog up A&E. Ambulances fume outside hospitals, unable to disgorge their patients because hospital beds are full of frail elderly people with nowhere to go. Routine operations are cancelled. Staff trudge grimly through hellish scenes and the rest of us worry about falling ill. We are all equal in the face of turmoil.
Does the NHS need more money? Yes, if it is to go on providing all the services people expect. The strains on A&E are eating up resources that should have been used for reform. Either we find more money, perhaps through a dedicated tax, or the prime minister must have a grown-up conversation with the public about what is possible.
Should we keep performing complex operations on old people with a low chance of survival? (Many doctors think we should not.) Should over-the-counter remedies such as paracetamol be free on prescription? Can we afford expensive drugs that prolong life by a few weeks? What is going to give?
Theresa May attempted to face the public with some uncomfortable facts last year, with her manifesto pledge to make people pay more for social care. But it was less of a conversation than a bombshell. The cack-handed way in which it was sprung on the public backfired spectacularly. A grown-up conversation about healthcare needs a long run-up and a grown-up opposition. It may even need a royal commission involving all the former Labour, Liberal Democrat and Conservative health ministers who privately agree on almost everything, while their parties fill the media pretending otherwise.
Instead, we get small amounts of new money to prop up ailing services. We get a slow, disorderly rationing of things by managers whose job is to make ends meet, not to work out — for example — how much a physiotherapist might save the whole NHS if she helped an elderly person who would otherwise never get out of bed again.
And here’s the real problem. The system doesn’t put the physios where they are most needed, because the system isn’t a system at all. The NHS is not the monolith of popular imagination, but an alphabet soup of 700 different organisations: acute hospital trusts, mental health trusts and regulators — plus 8,000 GP surgeries in England and Wales. It is a ramshackle lifeboat held together with dotted lines and goodwill.
When my father was admitted to hospital two years ago, a succession of staff came to ask us questions. What medicines was he taking? Had he been ill before? Did he live alone? He was in no state to answer. It took five days for the hospital to get his medical records, because in England your medical records are held by your GP. We must be almost the only civilised country in the world where you can black out in your own home and fetch up in your local hospital and be treated as though you have dropped in from Mars when you have lived in the same town for 50 years and paid taxes all your life.
That’s not the only divide. The reluctance of many GPs to visit care homes adds to A&E visits, because residents whose early symptoms were not treated are rushed to hospital after they fall over or fall ill. And the strains on “community services” mean elderly patients remain stuck in a hospital bed because there is no one to dress their wound, or give them chemotherapy, outside.
Community services — cottage hospitals, district nurses, occupational therapists — are the invisible glue holding up the edifice. But the obsession with the numbers of hospital nurses and doctors — which the government has kept increasing — means that little attention has been paid to the virtual halving in expert local nurses in a decade.
Money follows power. And power lies with the chief executives who run the big hospitals. Outside Northumbria and Salford, few hospital trusts run community services, so they don’t have an immediate financial interest in supporting them.
To bridge these divides, governments have spawned endless agencies: clinical commissioning groups, primary care trusts, Healthwatch. They have tried to limit monopoly power. But in our desire to avoid monopolies we have ended up with a bureaucracy in which the payments made by different health fiefdoms to each other cost anywhere between 4% and 14% (depending on whom you talk to) of the entire NHS budget.
I have observed the NHS for more than 10 years: as a journalist, as a non-executive director of the NHS regulator Care Quality Commission, as a patient and relative, and as head of David Cameron’s policy unit in No 10. Unlike many patients, I have a map. Yet like many patients, I can still feel lost. There are more job titles in the NHS than in many multinational corporations — some of them jobs that exist simply to tie together the disparate pieces.
What if we really had one truly unified national medical system?
What if GPs were based in hospitals with access to CT scanners, instead of having to write a letter to a consultant asking for a test in four weeks’ time?
What if hospitals ran community services, so they could see the need to hire district nurses? What if patients could go to one place, tell one story, and see the pharmacist at the same time?
Until we have one united medical system, we will have to rely on “goodwill” alone. But “goodwill” soaks up enormous amounts of time. I meet brilliant doctors and nurses, who seem to spend half their time in well-meaning committees.
What strikes me is how many NHS leaders are trying to bridge divides. The GPs who have persuaded hospitals to let them open clinics in A&E. The heads of hospital trusts, in places such as Northumbria and Greater Manchester, who are taking over GP practices and community services.
Simon Stevens, the NHS England chief executive, is encouraging this. But he needs to be more prescriptive. Every A&E should have a GP surgery with proper diagnostic equipment. All GPs should be salaried (half already are). Hospitals should run community services.
Some readers will worry I am proposing some kind of Stalinist NHS that would hold taxpayers to ransom. Perhaps I am; but the current system isn’t working. Others may think I am just shuffling deckchairs, when what is needed is cold hard cash. I agree more cash is needed. But it is not just about making economies, real or false. As Professor Sir Mike Richards, the cancer expert and former chief inspector of hospitals, is fond of saying: “The cheapest way to look after a patient is to diagnose them the day before they die.”
Whatever happens this winter, I do believe the NHS needs more money. But I would pay it to those who can create a unified medical system. One system that doesn’t pay people to ask you the same questions again and again, but treats you early and gets you out of hospital because it works off one budget. One system, which means that none of us ever need to be lost in the NHS without a map, ever again.

